 华亿体育(中国)游戏平台
华亿体育(中国)游戏平台JACI:过敏性肺炎:吸入多种抗原引起的纤维性肺泡炎
发布日期:2019-04-30
原标题:过敏性肺炎:吸入多种抗原引起的纤维性肺泡炎
延伸阅读
JACI
https://doi.org/10.1016/j.jaci.2018.09.040
Abstract:
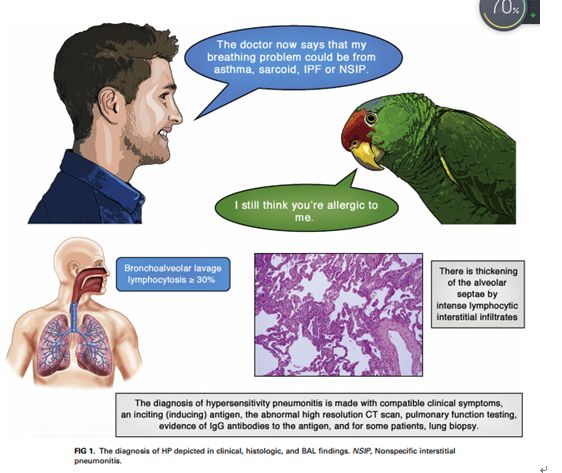
Hypersensitivity pneumonitis (HP) is a TH1 lymphocyte–biased fibrosing alveolitis caused by antigens ranging from avian excreta, fungi, thermophilic bacteria, and protozoa to reactive chemicals found in the workplace. Mimicking a viral syndrome, acute exposures to inciting antigens cause abrupt onset of nonproductive cough, dyspnea, and chills with arthralgias or malaise usually from 4 to 8 hours later so that the temporal relationship between antigen exposure and symptoms might be unsuspected. The histology of HP reveals prominent lymphocyte infiltrates that thicken the alveolar septa with poorly formed granulomas or giant cells. Bronchoalveolar lavage fluid demonstrates greater than 20% lymphocytes in nearly all patients. Abnormalities on high-resolution computed tomographic examinations range from nodular centrilobular opacities in acute/subacute disease to increased reticular markings and honeycombing fibrosis, which typically are predominant in the upper lobes, in patients with advanced disease. Descriptors include “mosaic” attenuation and ground-glass opacities. Repeated episodes can result in nodular pulmonary infiltrates and suspected nonspecific interstitial pneumonia or idiopathic pulmonary fibrosis. Clinicians require a high level of suspicion to make an early diagnosis of HP before extensive pulmonary fibrosis or restrictive lung disease has occurred.an expert panel of the American Thoracic Society commented that, ‘‘For patients with suspected interstitial lung disease in whom BAL is performed, we suggest that lymphocyte subset analysis NOT be a routine component of BAL cellular analysis.’’ What constitutes a ‘‘high level of confidence’’ in diagnosis is a matter of debate. In the absence of a diagnostic test, the diagnosis is made with compatible clinical symptoms, an inciting (inducing) antigen, an abnormal high-resolution computed tomographic (CT) scan, pulmonary function testing, evidence of IgG antibodies to the antigen, and, for some patients, lung biopsy.
Authors:
Paul A. GreenbergerMD

——浙大迪迅 译
过敏性肺炎(HP)是一种TH1淋巴细胞偏向性纤维性肺泡炎,由多种抗原引起,包括禽排泄物、真菌、嗜热细菌和原生动物,以及工作场所发现的反应性化学物质。与病毒综合征相似,急性暴露于刺激抗原可导致突然出现无生产能力的咳嗽、呼吸困难、伴有关节痛的寒战或不 适,通常在4至8小时后发生,因此抗原暴露与症状之间的时间关系可能没有受到怀疑。HP组织学表现为明显的淋巴细胞浸润,使肺泡间隔增厚,伴有肉芽肿或巨细胞。几乎所有患者的支气管肺泡灌洗液中淋巴细胞都超过20%。高分辨率计算机断层检查的异常情况:从急性/亚急性疾病的结节性小叶中心混浊到晚期疾病患者典型的以上叶为主的网状斑纹和蜂窝状纤维化。描述词汇包括“镶嵌样”衰减和毛玻璃混浊。反复发作可导致结节性肺浸润和可疑的非特异性间质性肺炎或特发性肺纤维化。在广泛的肺纤维化或限制性肺疾病发生之前,临床医生需要高度怀疑才能对HP做出早期诊断。美国胸科学会的一个专家小组评论道:“对于怀疑患有间质性肺病的患者进行BAL,我们建议淋巴细胞亚群分析不是BAL细胞分析的常规组成部分。什么构成了对诊断的“高度自信”是一个有争议的问题。在没有诊断试验的情况下,诊断需符合临床症状、刺激(诱导)抗原、异常高分辨率计算机断层扫描(CT)、肺功能检测、抗原特异性IgG抗体的证据、部分患者需肺活检。
延伸阅读
JACI
[IF:13.1]
Hypersensitivity pneumonitis: A fibrosing alveolitis produced by inhalation of diverse antigenshttps://doi.org/10.1016/j.jaci.2018.09.040
Abstract:
Hypersensitivity pneumonitis (HP) is a TH1 lymphocyte–biased fibrosing alveolitis caused by antigens ranging from avian excreta, fungi, thermophilic bacteria, and protozoa to reactive chemicals found in the workplace. Mimicking a viral syndrome, acute exposures to inciting antigens cause abrupt onset of nonproductive cough, dyspnea, and chills with arthralgias or malaise usually from 4 to 8 hours later so that the temporal relationship between antigen exposure and symptoms might be unsuspected. The histology of HP reveals prominent lymphocyte infiltrates that thicken the alveolar septa with poorly formed granulomas or giant cells. Bronchoalveolar lavage fluid demonstrates greater than 20% lymphocytes in nearly all patients. Abnormalities on high-resolution computed tomographic examinations range from nodular centrilobular opacities in acute/subacute disease to increased reticular markings and honeycombing fibrosis, which typically are predominant in the upper lobes, in patients with advanced disease. Descriptors include “mosaic” attenuation and ground-glass opacities. Repeated episodes can result in nodular pulmonary infiltrates and suspected nonspecific interstitial pneumonia or idiopathic pulmonary fibrosis. Clinicians require a high level of suspicion to make an early diagnosis of HP before extensive pulmonary fibrosis or restrictive lung disease has occurred.an expert panel of the American Thoracic Society commented that, ‘‘For patients with suspected interstitial lung disease in whom BAL is performed, we suggest that lymphocyte subset analysis NOT be a routine component of BAL cellular analysis.’’ What constitutes a ‘‘high level of confidence’’ in diagnosis is a matter of debate. In the absence of a diagnostic test, the diagnosis is made with compatible clinical symptoms, an inciting (inducing) antigen, an abnormal high-resolution computed tomographic (CT) scan, pulmonary function testing, evidence of IgG antibodies to the antigen, and, for some patients, lung biopsy.
Authors:
Paul A. GreenbergerMD
2019-4-16 Review
创建过敏性疾病的科研、科普知识交流平台,为过敏患者提供专业诊断、治疗、预防的共享平台。
地址:杭州市滨江区滨康路568号2号楼 电话:0571-87968248-805 网址:www.martscope.com
COPYRIGHT©2003-2024 www.martscope.com CORPORATION. ALL RIGHTS RESERVED
COPYRIGHT©2003-2024 www.martscope.com CORPORATION. ALL RIGHTS RESERVED


浙大迪迅
官方微信

MK手机投注 | 安博·体育(中国)有限公司-官网 | 乐动官方网站 | 星空手机版 | 星空手机版 | mk体育(MKsports集团)股份公司 | 安博手机网页版登录入口 | 华体平台 | 千亿体育官网在线登录入口中国有限公司 |